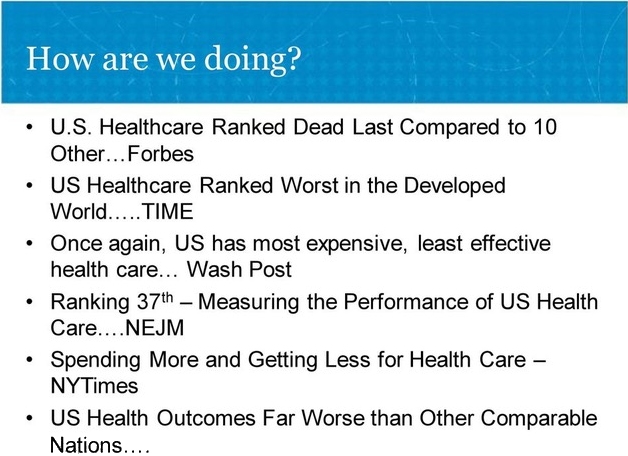
It’s time to think of all the reasons single payer, universal health care is the solution to America’s woeful, corporate healthcare. Yes, we all know that when ex-President Obama sold-out to his big-time contributors in the health care industry and the hedge and equity funds that control them, we were stuck with a health care boondoggle, popularly known as Obamacare (really a reprise of RomneyCare), that leaves twenty-nine million Americans uninsured, vastly more underinsured and all unhappy. And that’s not counting the millions more in danger of bankruptcy because of medical bills (still the leading cause of bankruptcy in the U.S.).
From the beginning and gaining momentum as the years passed, plans offered on state-wide federal exchanges (for those not in employee health plans) increasingly limited access to medical providers and dramatically raised costs. Total healthcare spending in 2017 (last year for which figures are currently available) topped out at $3.5 trillion, a 4% increase over 2016. Health care spending per person came in at an eye-popping $10,739. With premiums rising along with deductibles (amount patient has to pay before insurance kicks in), it was no surprise that in 2019 when Trump lifted the coverage mandate, 400,000 formerly insured “just said no.”
This coming year, the average premium (not counting those eligible for subsidies) hovers around $612 per month ($7,344 for the year). Add in a $4,000 deductible on the most popular plan (silver) and when your insurance kicks in —after you have spent $11,000 — you’re not home free. Only 70% of your medical expenses will be picked up. You’re still on the hook for 30%. Prices get wilder and crazier (deductibles over $6.000) if your finances force you to select a plan with a cheaper premium.
Welcome to corporate healthcare where profits are king and patients are the road to riches. In service to that ideal, the ever-inventive medical power brokers have come up with new wrinkles to delude the patient population into believing that more (traditional drug-and procedure-saturated medicine) is better —ignoring the reality that life expectancy in the U.S. has been dropping for two straight years. They dismiss reasonably priced healthcare options as “junk science (acupuncture, massage, chiropractic care). Sometimes they take patient choice completely out of the equation.
| Arthur W. saw a neurologist in a big medical group affiliated with a major hospital. He decided to see another neurologist in the same practice. When he called to make the appointment, he was told that he would not be able to see the neurologist of his choice since he had already seen a neurologist in that practice. Arthur was outraged but decided against pursuing his complaint. He was afraid the medical practice would drop him. He ended up making a repeat visit to a provider he neither liked nor trusted. |
What happened to Arthur happens more often these days as medical practices get bigger and scoop up more and more doctors in the same specialty. If you don’t like your doctor, the practice threatens, you can hit the road, a step patients are usually reluctant to take. Realizing that most Americans, particularly those millions forced into second or third jobs to pay their medical expenses or college loans, don’t have the time or energy to do the arduous work a transfer entails, owners of medical practices aren’t overly concerned about losing patients. After all for most patients “better the devil you know than the devil you don’t.”
The bottom line: U.S. healthcare has taken two critical components of a patient-centric system —access and choice — off the table. Like other corporations, medical practices these days slap an LLC (limited liability company) behind their names and suddenly are endowed with a lower level of liability for their actions (medical malpractice may still apply to individual doctors, but the owners of the practice have no personal legal liability). In most states, LLC practices also shield their owners from the tax burdens assessed on non-LLC corporations. Another tax dodge for corporate America.

| It was a nightmare scenario. Henry G. had been operated on for advanced bladder cancer and now used a catheter. Having come down with a bladder infection, a usual occurrence after his surgery, he called to make an appointment with the urologist who had been taking care of him through his surgery and beyond. He was told that his doctor no longer worked at the practice and the practice would not divulge where his doctor had gone. Henry was blindsided ‘What do I do now?’” |
Henry was stuck between a rock and a hard place. As it turned out, his doctor had been fired by his practice (not bringing in enough business is the usual cause for termination or violating the strict time caps —7-11 minutes —for each patient visit) and started a new urology practice with colleagues who had been similarly booted. But even if Henry had managed to find his doctor, he probably couldn’t have scheduled a visit. Under the terms of the contract his doctor signed with his former employer, he was bound by a restrictive covenant clause that barred him from treating former patients or even from practicing within thirty-five miles of his former employer.
How prevalent are these restrictive covenants? In a recent survey of two thousand PCPs (primary care physicians) in five states, 45% admitted to being bound by a non-compete clause. Wresting a doctor away from long-time patients, particularly those with chronic conditions, is devastating for patients. It happened to one long-term cancer survivor. She received a letter from her doctor’s medical practice announcing the doctor’s exit but omitting reference to his new practice. Her response— “Somehow they [the practice enforcing the non-compete clause] lost sight of patient care and were more concerned about the bottom line.
That goes for the entire healthcare industry which has steadily relegated patient care to the bottom of the priority list. On top —profits, the bigger, the better. “When doctors want to move from one practice to another, if they’ve got a good therapeutic relationship with their patients, you’d think that public policy would want them to continue to treat those patients that trust them” (Judy Conti, National Employment Law Project). Ah, that’s the rub, isn’t it? When “public policy” clashes with profit-driven capitalism, the pillage and plunder metrics of capitalism invariably win out.
To defend the indefensible, big wigs at major healthcare practices pretend that non-compete clauses actually benefit patients — “…because they [non-compete clauses] provide stability with a practice and ensure continuity of care.” (chief poobah of a major Iowa clinic). Not convinced? Try this excuse on for size— “Patients get frustrated but what they may not understand is that this is a legal thing that we have to abide by.” (Spokesperson for the University of Wisconsin health care system). As you can see, a major component of the success of non-compete clauses is the lack of moral courage on the part of those who feel bound to enforce them. How about the doctors’ “natural allies,” the AMA (American Medical Association)? As the official lobby for corporate medicine, not individual doctors, their allegiance is to the power brokers — in a carefully nuanced statement, Dr. Patrice Harris, President-elect dithered — “To the extent that these agreements disrupt continuity of care, this is of great concern to the AMA.”
What are the chances a group of doctors bringing a lawsuit challenging both terminations and restrictive covenant clauses in medical contracts will prevail? Very good, according to David Clark, an expert on the legality of healthcare non-compete clauses — “No court is going to deny a patient who wants to go see a doctor of her choice.”
If you live in Massachusetts or Colorado, rejoice! If you don’t and have a chronic medical condition, consider moving. In these states (others are joining their ranks) although non-compete clauses in employment contracts are legal, the states’ judiciary will not enforce them against doctors.
By this time, it should be clear that In the U.S. plutocracy, patients are little more than victims of free market capitalism. Their needs are not being met and they are needlessly dying from neglect, medical screw-ups and shoddy care. Profit-driven healthcare is not the answer to a long, healthy life.
In later articles, Suspicious Angels will cover many other get-rich-quick healthcare scams flying under the radar. To give you a little taste of horrors to come, what about the advent of Electronic Health Records (EHRs), billed as the one sure way for patients to receive the most effective treatments, reduce medical errors, and provide a fast and efficient way to share their medical histories with doctors and hospitals virtually anywhere in the world. These wildly exaggerated claims convinced Obama to make them part of Obamacare. So far the feds have poured $36 billion into the EHR industry and made a lot of fat cats fatter. What have patients gotten in return — an error-prone, cumbersome system whose requirements vitiate doctor-patient interactions, making them little more than a fill-in-the-blanks exercise. Here’s how one administrator at a large medical center described a typical office visit in the era of EHRs —In America, we have 11 minutes to see a patient and [our doctors have] to be empathetic, make eye contact, enter about 100 pieces of data, and never commit malpractice. It’s not possible” (John Halamka)
But when it comes to outright larceny, “surprise billing” takes the cake. Let’s say you go to a hospital that’s part of your insurance company’s network, only to receive care without your knowledge or permission from a doctor who isn’t part of that network.
| Charlotte C. was forced to have an emergency C section. Although the hospital was in her insurer’s network, an in-network anesthesiologist wasn’t available, so she was billed $15,000 for the out-of-network doctor who replaced her. |
Was she legally obligated to pay? You betcha! We’ll give you all the gory details in a later article.
There’s an even darker side to U.S. healthcare. “Predictive medicine” (not unlike predictive policing) helps insurers predict how likely you are to develop specific illnesses and more important, from the doctor’s point of view, how likely you are to pay what your insurer doesn’t cover. As high deductibles force patients (both those insured by their employers and those buying insurance on the federal marketplaces) into paying a greater share of the larcenous fees doctors and hospitals charge, health providers want to know how likely they are to be paid before they treat you. It falls to a couple of companies to get the goods on your payment history.
Healthcare in America hasn’t always been so blatantly market-oriented. Fifty-eight years ago, this dedication celebrating the commitment of the U.S. medical system to the welfare of patients appeared at the end of the movie The Young Doctors —
| “This film is dedicated to the medical profession for its constant devoted service to mankind.” |
Little more than a half century later, it’s hard to imagine that U.S. medicine ever operated that way. Watch the movie (it’s on YouTube) and weep for what has been sacrificed in the name of profits.

What will it take to unseat the power brokers who control healthcare in America? Lots of us united around one goal — single payer universal healthcare.
| Small acts, when multiplied by millions of people, can quietly become a power no government can suppress, a power that can transform the world.” (Howard Zinn) |
2,231 total views, 1 views today